


Norwegian All-Cause Vaccination Study Does NOT Show mRNA Vaccines are Safe & Effective!
The implied conclusions of this recent study lack concrete evidence and sufficient methodology to establish the safe & effective claim!

A recent Norwegian study on all-cause mortality by vaccination status indicates that their findings establish the fact that the COVID-19 mRNA vaccines are safe and effective!

I disagree with these findings because they lack concrete evidence and sufficient methodology.
Here are my detailed comments:
1. Healthy User Bias
The analysis suggests that the lower mortality rate in vaccinated cohorts, as evidenced by the hazard ratio (IRR), may indicate a causal relationship with COVID-19 vaccination. However, the observed lower IRR in individuals with 3+ doses compared to those with 1-2 doses strongly suggests the influence of healthy user bias—a self-selection effect where health-conscious individuals are more likely to get vaccinated and maintain healthier lifestyles overall.
2. Lack of a Time Series Analysis
The study would have benefited greatly from presenting time series data, such as weekly or monthly mortality rates by vaccine dose. A temporal view would provide insights into how mortality rates fluctuate over time in relation to vaccination campaigns, pandemic waves, and other external factors. This is particularly important for understanding potential lagged effects or temporal biases.
3. Crude Age-Banding
The use of broad age groups limits the granularity of the analysis and may obscure differences in mortality risk across finer age brackets. Incorporating more detailed age stratification could enhance the precision and interpretability of the results. A blended age-standardized rate was not provided.
4. Misleading Comparisons
In the introduction, the study states: “Most countries worldwide have experienced excess mortality that coincides temporally with the COVID-19 mass vaccination campaigns. This has led to speculation on the potential long-term effects of the vaccines on mortality risk.” While this is an important concern, the analysis does not provide sufficient evidence to determine whether vaccinated individuals experienced lower (or higher) mortality compared to what they would have experienced with a placebo or no vaccination. (The methodology also does not address the temporal correlation; lack of time series analysis) The comparison of vaccinated versus unvaccinated individuals alone cannot fully disentangle the effect of vaccination from other underlying factors, such as baseline health differences or confounders.
5. Contextual Trends in Norway
The analysis could have benefited from situating the findings within broader national mortality trends. For example, data from Norway show no statistically significant excess mortality compared to the 2017-2019 baseline, as per Mortality Watch. Excess mortality remained within the 95% prediction intervals (PI) during the pandemic years:
2020: -4.1% [-8.7%, 0.4%]
2021: -2.9% [-7.4%, 1.7%]
2022: 3.4% [-1.1%, 8.0%]
2023: -3.3% [-7.8%, 1.3%]

These data highlight the importance of contextualizing results against national trends. For Norway, this suggests that mortality patterns during the pandemic largely remained within expected ranges, making causal claims about vaccination’s impact doubtful. Moreover, Norway did not appear to experience any significant excess mortality during the peak of the pandemic. The slight increase in 2022 might simply be a result of a “catch-up” effect or a lingering negative impact of the pandemic response.
6. Alternative Methodology
The authors adjusted for several confounding variables, including sex, calendar time, county of residence, and risk group status. However, an alternative approach could involve historical matching or synthetic control. By comparing vaccinated individuals’ mortality rates to historical mortality rates of individuals with identical attributes (e.g., matched on sex, age, risk group, and residence), they could have established a counterfactual baseline. This methodology would help mitigate biases and provide a more robust assessment of vaccination’s impact on mortality. Conclusion While the study addresses a crucial research question, I believe it lacks sufficient evidence to establish a net positive effect of vaccination or its safety. The absence of a time series analysis further hinders the validity and impact of the findings. To address these methodological and interpretational gaps, I suggest incorporating a time series analysis with a historically matched baseline.
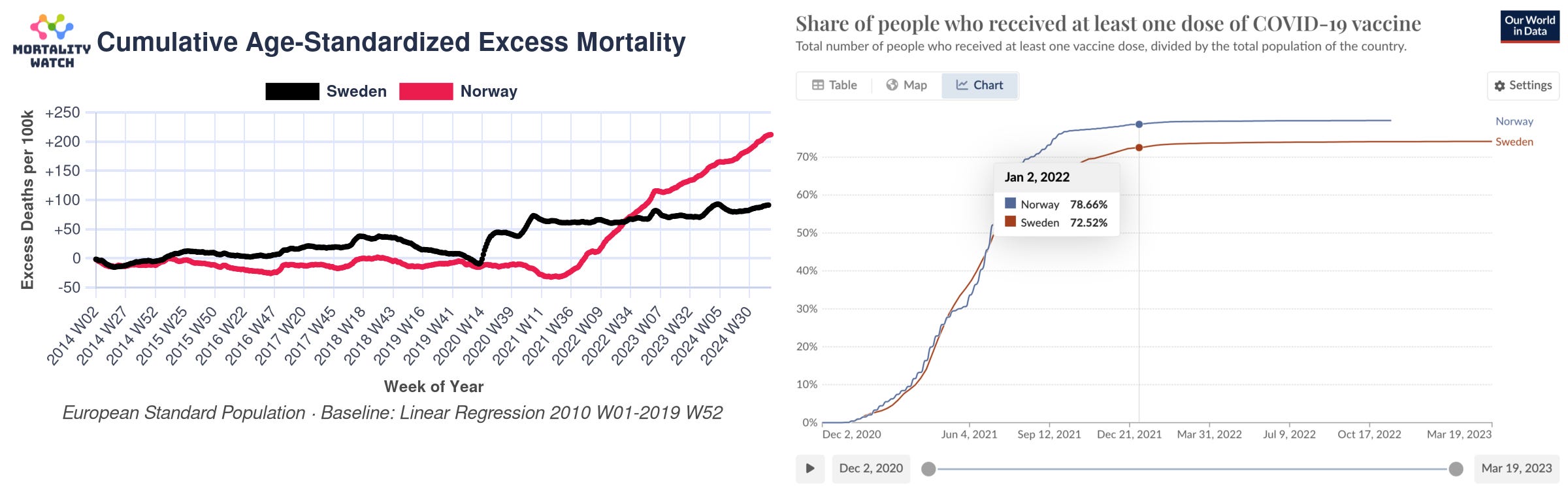
7. Sweden vs. Norway
Epidemiological evidence from comparing Sweden and Norway directly contradicts the notion that these vaccines are both “safe and effective”. Despite having a higher vaccination rate, Norway experienced higher excess mortality compared to Sweden, in 2022, after vaccination!
8. Lack of Transparency in Model Calculations
The calculations used in the model are not publicly disclosed. This especially leaves the exact method for determining rates unclear. For instance, it is not specified how the rate for the unvaccinated group was calculated. If the unvaccinated population (denominator) was derived by subtracting the known vaccinated population from the total population, this residual group might not accurately represent the unvaccinated population. Such an approach introduces a risk of misclassification, where unconfirmed or unreported vaccinated individuals could be mistakenly included in the unvaccinated group. This misclassification risk is one-sided, potentially leading to over- or underrepresentation of the unvaccinated cohort. Additionally, no confidence intervals (CI’s) were provided to account for this uncertainty, further limiting the reliability of the conclusions.
9. Absence of Stratification by COVID-19 and Non-COVID-19 Mortality
The data were not stratified to differentiate between COVID-19-related and non-COVID-19-related mortality. Such stratification is essential for a more rigorous estimation of the potential effects of COVID-19 vaccination and to address other issues, such as attribution bias and possible over- or undercounting of deaths. By isolating non-COVID-19 mortality, it becomes possible to better assess confounding factors that primarily affect this category. Additionally, examining changes over time could offer valuable insights into whether vaccination has a protective or harmful effect, while also highlighting trends that might otherwise remain obscured.
10. Exclusion of Data for Cross-Vaccinated Individuals
The dataset completely removed (“censored”) cross-vaccinated individuals without providing a clear rationale. This lack of explanation raises questions about the potential impact of this exclusion on the results, and whether it could introduce bias or reduce the generalizability of the findings.
11. Population Data of Study Appears 7% Higher than Adult Population from Stats Norway Indicates!
The population data in the study appears to be incomplete or inconsistent.
The study reports: “The study included 4,645,910 individuals (49.8% women) with 132,963 deaths during follow-up.”
DEATHS:
I couldn't find deaths by single year ages at Stats Norway; but I found it at Eurostat, however 2023 is not posted, thus I simply doubled 2022 (to account for 2023):
Thus reported deaths for 18+ sum to 41,781 + 45,570 + 45,570 = 132,921 which is roughly in line with what the study reports.
POPULATION:
Similarly, the mean population 18+ calculated as (4,279,679+4,316,747+4,376,793)/3 = 4,324,406 from Stats Norway is 6.9% lower than what the study reports.
It is possible that the 7% difference may be explained by "lost to follow up" (death, migration, etc.) - however that seems quite high, and it remains unknown if this disproportionately affects the unvaccinated cohort in the rates calculations.
The discrepancy in the population figures are unexplained and raise significant concerns about the accuracy and reliability of the study’s findings.
12. Conclusion
The authors’ conclusion, “In conclusion, there was a reduced rate of death among individuals vaccinated with mRNA vaccines during 2021-2023 in Norway,” is clearly flawed. This conclusion was drawn by comparing the mortality rates of vaccinated individuals to those of the unvaccinated cohort. However, as outlined in the 10 points above, this approach is severely flawed and lacks proper scientific rigor. Such a conclusion cannot be legitimately inferred.
What the study actually demonstrates is that the mortality rate in the self-selected vaccinated cohort appears lower, primarily due to confounding factors. The unvaccinated cohort represents the remainder of the population, including individuals at the end of life receiving palliative care, who were unlikely to receive vaccination.
A proper comparison would require establishing a baseline mortality rate for the vaccinated cohort using historical, cohort-specific data that accounts for confounders. Only by comparing the observed mortality rate against this true baseline could one accurately determine whether the rate among vaccinated individuals is genuinely lower or higher.
Note: 7-12 were added after the initial publication of this article.
I have sent this friendly letter, which includes most of this feedback, to the authors:

Please let me know your thoughts in the comments!
Very nicely done criticism, and important comments about interpretation of vaccination-status mortality!
Do we have the isolation and purification of this new bird flu?
Avian flu virus H5N1: No proof for existence, pathogenicity, or pandemic potential; non-“H5N1” causation omitted
nlm.nih.gov
More fakery from the wizards
Moderna CEO Stéphane Bancel Says They ‘Copied & Pasted’ the Spike Sequence From the Chinese Government
https://open.substack.com/pub/lionessofjudah/p/moderna-ceo-we-never-had-access-to?r=145evj&utm_medium=ios
Do we have the isolation and purification documents of Covid 19 it appears it never existed?
FOIs reveal that health/science institutions around the world (225 and counting!) have no record of SARS-COV-2 isolation/purification, anywhere, ever
https://www.fluoridefreepeel.ca/fois-reveal-that-health-science-institutions-around-the-world-have-no-record-of-sars-cov-2-isolation-purification/
They knew contagion didn't exist after the 1923 Lancaster Study, but they continued to push the fear narrative to keep a control on humanity.
https://en.rattibha.com/thread/1629159544348717061
ABOUT A YEAR INTO THE KANSAS FLU A STUDY CAME OUT CALLED THE THE
LANDMARK STUDY OF MILTON J.
ROSENAU, MD, "EXPERIMENTS TO DETERMINE MODE OF SPREAD OF INFLUENZA," WAS PUBLISHED IN THE JOURNAL OF THE AMERICAN MEDICAL
ASSOCIATION IN 1919.
https://www.ggarchives.com/Influenza/TheRosenauExperiment-1918-1919.html